
Understanding Fractures: Healing, Pain, Non-Unions, and Ultrasound Therapy
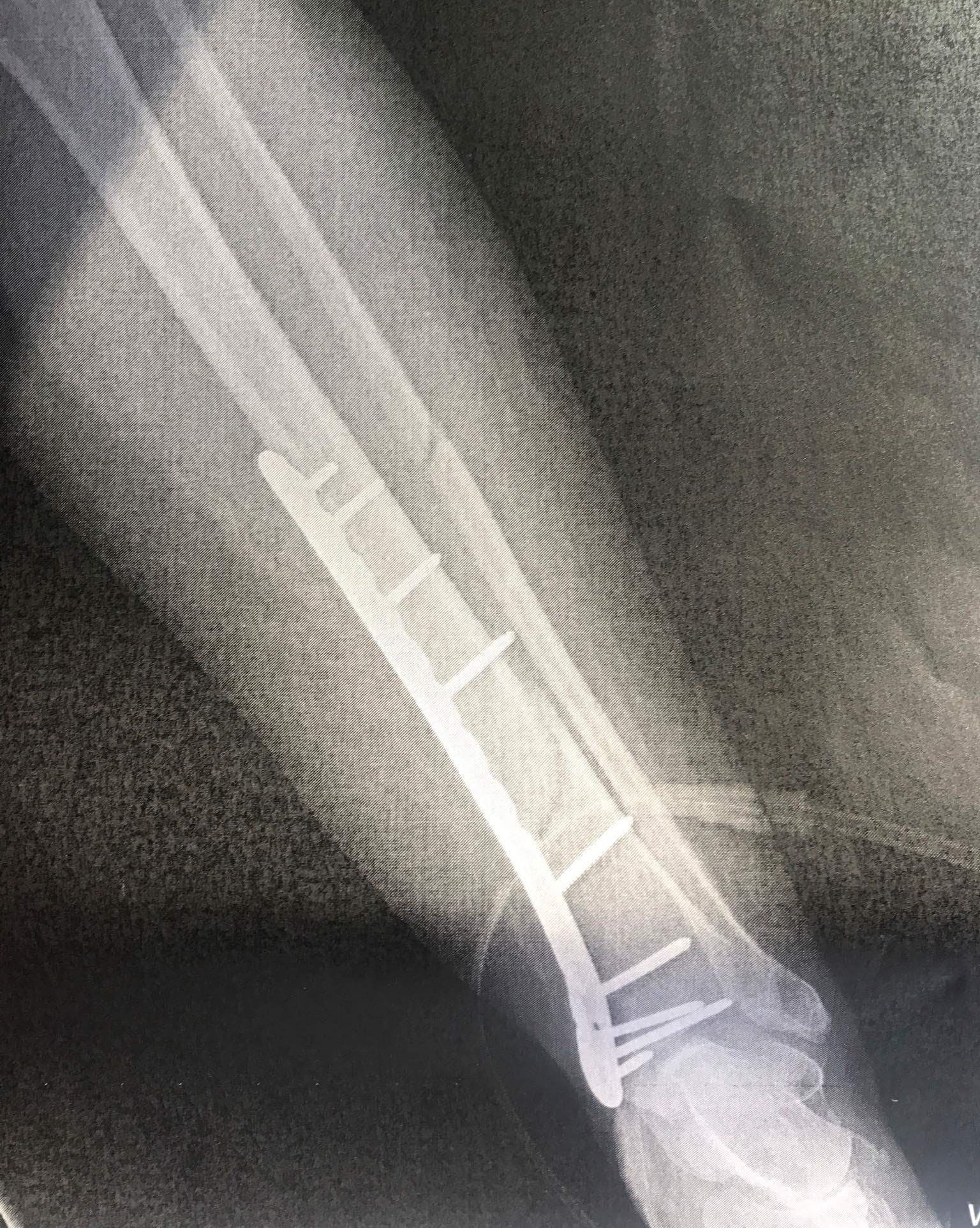
After 50 years of avoiding broken bones, I slipped on a single ceramic tile during a trip to France and broke both my tibia and fibula. The local hospital staff were amazing. Following a temporary overnight cast, I underwent an Open Reduction and Internal Fixation (ORIF) surgery, where my complicated spiral tibia fracture was secured with a plate and 10 pins.
Unfortunately, after four months recovering at home in Worcestershire, I was diagnosed with a non-union fracture. Thankfully, my lovely orthopaedic consultant in Cheltenham suggested we try Exogen ® Ultrasound Bone Healing treatment. I am thrilled to say it was a success. After three months of daily treatment, "cotton-wool-like" growth was visible in the (quite large) gap on my X-ray. After a further three months, I was completely healed. I was incredibly relieved to avoid further surgery, which would have required a bone graft from my hip.
Ultrasound bone healing machines are particularly well known for assisting non-union fracture healing, as well as accelerating recovery in fresh breaks. In the comfort of your own home, you can use an ultrasound device for just 20 minutes a day.
The Biology of Bone Fracture Healing
Bone fracture healing is a complex, continuous biological process. It must happen in a specific order to successfully rebuild the bone.
1. Hematoma Formation (Days 1–5): When a bone breaks, blood vessels rupture, causing blood to pool and clot at the fracture site. This clot (hematoma) forms a structural framework that stops further bleeding and provides a base for new tissue to grow. Key cells: Platelets and phagocytes (which clean up dead tissue and debris).
2. Inflammation (Days 5–11): The body mounts an intense localised immune response. The area becomes swollen, red, and painful as blood flow increases to deliver essential nutrients, oxygen, and specialsed cells to begin the repair process. Key cells: Macrophages, white blood cells, and mesenchymal stem cells.
3. Soft Callus Formation (Weeks 2–3): The inflammatory cells are replaced by granulation tissue. Blood vessels begin to regrow, and the body creates a "soft callus" made of fibrous tissue and cartilage to act as a temporary splint bridging the broken bone ends together. Key cells: Fibroblasts and chondroblasts.
4. Hard Callus Formation (Weeks 3–12): The soft, cartilaginous callus is gradually replaced by woven, immature bone through a process called endochondral ossification. This hard callus acts as a rigid, bony bridge that secures the fracture. Key cells: Osteoblasts (bone-forming cells).
5. Bone Remodeling (Months to Years): The final and longest stage. The rigid woven bone is continuously broken down and reorganized into stronger, dense, mature lamellar bone, matching the original shape and structural strength. Key cells: Osteoclasts (bone-resorbing cells) and osteoblasts.


Understanding Fracture Pain
Post-fracture pain is the body's natural response to broken bones and damaged surrounding tissues (like muscles, nerves, and ligaments). It serves as your body's alarm system to protect the injured area. Discomfort naturally fluctuates from sharp, sudden aches right after the break to a dull, lingering soreness and stiffness during immobilisation.
Standard healing pain generally progresses through two phases:
Acute (1-7 days): Intense, immediate pain right after the break.
Sub-acute (2-6 weeks): Dull, aching pain during the healing weeks.
Chronic Pain occurs when pain persists beyond normal healing time (typically >3 months) even after the bone has healed. It is frequently triggered by overactivity, weather changes, and scar tissue stiffness rather than direct bone movement. It is often a dull, aching, or neuropathic pain that can occur at rest.
In contrast, if sudden spikes of pain return or worsen after the expected healing time has passed, this can signal a complication known as a Non-Union. This is characterised by localised tenderness, aching, and sharp mechanical pain that worsens when weight is applied or the limb is moved.
Non-union Fractures
A non-union fracture occurs when a broken bone fails to heal naturally or within the expected time frame. Instead of fusing together, the fracture site remains unstable. Biologically, a non-union is defined as a persistent failure of the bone to bridge with new bone after 9 months, or if there has been no progressive healing for 3 consecutive months.
Healing halts due to a breakdown in three physiological requirements: adequate blood supply, sufficient mechanical stability, and a robust cellular response. Non-union fractures are more likely if the bone breaks from a high-energy injury, such as from a motor vehicle collision, because severe injuries often disrupt blood supply to the broken bone.
Hypertrophic Non-Unions: Have abundant blood supply and biological activity but lack mechanical stability. The body attempts to heal by generating massive amounts of fibrous, cartilaginous "callus," which cannot bridge the gap because the bone segments are moving too much. Fixing the mechanical instability is typically the primary treatment.
Atrophic Non-Unions: Have poor blood supply and inadequate biological activity. The bone ends look "starved," lack callus formation, and the fracture gap is filled with inactive fibrous scar tissue. Treatment usually requires surgically stimulating the biology (e.g. bone grafting) and improving stability
Signs of a Non-Union
Aside from pain, signs that a fracture has not united include:
Tenderness and swelling directly at the break site.
A "giving way" sensation or abnormal movement where the bone should be rigid.
Visible limb or joint deformity.
Difficulty bearing weight or an inability to use the limb as expected.
Common Causes
Poor blood supply: Bone ends require blood and nutrients to rebuild tissue.
Infection: Bacteria at the fracture site can prevent proper regeneration.
Excessive movement: Moving the bone too early or cast/implant failure.
Underlying health issues: Severe diabetes, anemia, or the long-term use of certain medications (like anti-inflammatories) can suppress healing.
Non-Union Treatment
Unfortunately non-unions rarely heal without intervention.
The Non-invasive Option:
Ultrasound Bone Healing Stimulators: A small device is placed over the skin of the fracture site. It uses Low-Intensity Pulsed Ultrasound (LIPUS) waves to kick-start the biological bone-healing process. (You can search for ‘LIPUS’, ‘Exogen®’, or ‘Osteotron®’ for more information on how these machines work). Always take your orthopaedic consultant’s advice.
The Surgical Options:
Bone Grafting: Using bone from another part of the body or a donor to stimulate growth and seal the fracture.
Hardware Revision: Adjusting, tightening, or replacing surgical plates and screws to provide better stability.
Disclaimer: This information is for educational purposes. If you are experiencing unexplained, persistent pain following a bone fracture, please contact your doctor or an orthopaedic specialist for an evaluation and imaging.
NHS Funding Guidelines for Exogen® in the UK
The NHS sometimes provides the Exogen® Ultrasound Bone Healing System, but only under strict circumstances. The updated NICE MTG12 Guidance supports the use of Exogen® for long bone fractures (like the femur, tibia, or humerus) that have failed to heal after 9 months. Clinical evidence demonstrates high healing rates and potential cost savings by preventing further surgery
NHS commissioning bodies and local Integrated Care Boards (ICBs) routinely adopt this guidance, but they enforce strict clinical criteria. To be eligible for NHS-funded Exogen® therapy, patients typically must meet the following parameters:
Patient Profile: Must be aged 18 or older.
Fracture Type: Applies to stable, un-displaced long bone fractures (e.g., tibia, femur, radius, ulna, or humerus).
Timeline: Non-union must be confirmed (failure to heal after 9 months).
Gap Limitations: The fracture gap must be 1 cm or less.
Exclusions: It is not commissioned for use in cases of infection, fractures caused by bone cancer, skeletal immaturity (children/adolescents), or during pregnancy.
For precise details regarding your local NHS trust's prescribing policies, please consult them directly.